Content discussed in this post
What syphilis is and why it matters now
How transmission happens: kissing, sexuality, and oral sex
Symptoms by stage: primary, secondary, and tertiary
Latency, neurosyphilis, and congenital syphilis
Tests: when to test, window period, and false positives
Treatment: simple regimens and follow-up
Prevention and partner care
Quick FAQ
Important notice (health disclaimer)
References and recommended reading
What syphilis is and why it matters now
Syphilis is a sexually transmitted infection caused by the bacterium Treponema pallidum. It has well-defined phases, can remain silent for long periods, and returns more severely if untreated. The key takeaway: syphilis does not go away on its own. Without treatment, it progresses and may affect the heart, brain, and nerves, with serious complications in pregnancy and for newborns.
How transmission happens: kissing, sexuality, and oral sex
Transmission occurs through direct contact with infectious lesions on mucosa or skin. This includes vaginal and anal sex, and also oral sex. Syphilis can be acquired through oral–genital contact alone if there is a lesion in the mouth, lips, or throat, or on a partner’s genitals. Kissing can transmit infection when there is an active oral or mucosal lesion. Vertical transmission can occur during pregnancy if the mother is infected and untreated.
Condoms and barriers (external or internal condoms and dental dams) reduce risk, though not completely, since lesions may be in uncovered areas. Avoid sexual activity during sores or prodromal symptoms and seek early evaluation to sharply reduce transmission.
Symptoms by stage: primary, secondary, and tertiary
Clinical evolution varies, but there is a typical path.
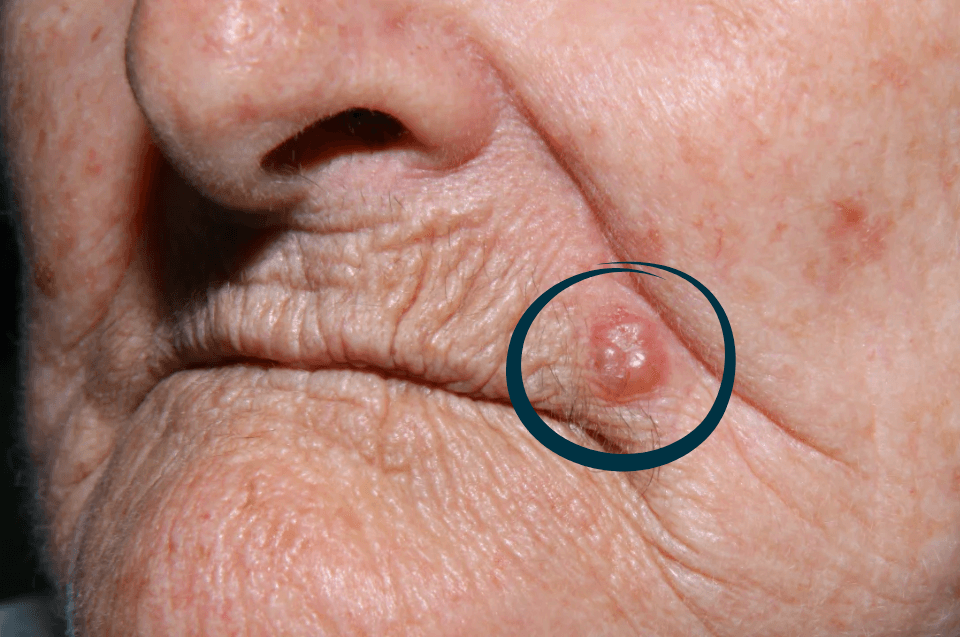
Primary syphilis
Usually appears 10 to 90 days after exposure. A hard chancre forms, typically a single, firm, well-demarcated ulcer that is usually not very painful at the site where bacteria entered (genitals, anus, mouth). Regional lymph nodes often enlarge. Even without treatment, the sore heals within weeks, which gives a false impression of cure. The infection persists.
Secondary syphilis
Weeks to months later, the bacteria have disseminated and systemic signs appear: a diffuse rash that often involves the palms and soles, condyloma lata in moist areas (wart-like lesions that are highly contagious), mucous patches, patchy hair loss, low-grade fever, malaise, and generalized lymphadenopathy. This phase improves spontaneously, but disease continues.
Tertiary syphilis
Years later, if untreated, deeper organs may be involved. Notable forms include:
Cardiovascular: syphilitic aortitis with risk of aortic dilation and insufficiency
Gummatous disease: granulomatous lesions in skin, bone, and viscera that can destroy tissue
Late neurologic disease: cognitive and behavioral changes, gait disturbance, and neuropathic pain from spinal cord and nerve involvement
This stage is serious and can cause permanent sequelae. The message is clear: early diagnosis and treatment prevent tertiary disease.
Latency, neurosyphilis, and congenital syphilis
After the secondary phase, infection enters latency. There are no symptoms, but tests remain reactive. Latency can be early (under one year) or late (over one year). Neurosyphilis can occur at any stage, including early, causing meningitis, uveitis, hearing loss, visual changes, and paresthesias. In pregnancy, untreated infection can result in congenital syphilis, with miscarriage, stillbirth, prematurity, or severe neonatal disease. This is why prenatal screening and immediate treatment when needed are essential.
Tests: when to test, window period, and false positives
Tests are divided into nontreponemal and treponemal.
Nontreponemal tests: VDRL and RPR. Quantitative, used for initial diagnosis and follow-up. Numerical titers fall with successful treatment.
Treponemal tests: assays such as EIA/CLIA, FTA-ABS, and TP-PA. Qualitative, confirm exposure, and tend to remain reactive for many years.
When to test
Test if there is a genital ulcer, suspicious rash, unexplained lymphadenopathy, high-risk sexual exposure, a partner diagnosed with syphilis, and in pregnancy screening programs. After recent exposure there is a window period. It can take two to six weeks for detectable antibodies to appear. If the initial test is negative but suspicion is high, repeat in 2 to 4 weeks or as advised by a clinician.
False positives and other pitfalls
Nontreponemal tests can yield false positives in pregnancy, autoimmune diseases, viral infections, and even post-vaccination. Confirm with a treponemal test.
A false negative can occur due to the prozone effect when titers are very high. Experienced laboratories dilute the sample to check.
Previously treated people may remain treponemal-positive for years. In these cases, the nontreponemal titer (VDRL or RPR) and clinical history guide management.
Treatment: simple regimens and follow-up
Treatment is simple and highly effective, especially early on.
Early syphilis (primary, secondary, or early latent): benzathine penicillin G 2.4 million units intramuscularly, single dose.
Late latent or unknown duration: benzathine penicillin G 2.4 million units IM, once weekly for 3 weeks.
Neurosyphilis and ocular/otic syphilis: aqueous crystalline penicillin G intravenously per specific regimens.
Penicillin allergy: options such as doxycycline can be used in nonpregnant patients, but penicillin remains the gold standard. In pregnancy with penicillin allergy, desensitization is recommended so penicillin can be used.
Practical points
The Jarisch–Herxheimer reaction can occur in the first 24 hours after the first dose. It presents with fever, chills, and transient malaise. It is alarming but not an allergy.
Abstain from sexual activity until lesions have healed and for at least 7 days after the dose.
Follow nontreponemal titers (VDRL or RPR) at 6 and 12 months to verify a fourfold decline, for example from 1:32 to 1:8. Lack of decline or a rise suggests reinfection or the need for reassessment.
Partners from the previous 3 months to 1 year (depending on stage) should be notified and tested. Treating the partner network prevents ping-pong transmission.
Prevention and partner care
Use barriers in all sexual practices, including oral sex with a dental dam or a condom cut and used as an improvised barrier when needed.
Get regular STI testing if you have new partners or are in a non-monogamous relationship.
Discuss symptoms and recent exposures with partners and agree to pause sexual activity during lesions or prodromal symptoms.
During pregnancy, complete all screening on schedule and treat immediately if diagnosed.
Quick FAQ
Does syphilis resolve on its own?
No. Initial lesions may heal, but the bacterium persists. Without treatment, disease progresses.
Can I get syphilis from oral sex alone?
Yes. Oral–genital contact with infectious lesions or mucosa can transmit syphilis.
I had one positive and one negative test. Which one counts?
Tests serve different purposes. A single result does not tell the whole story. Confirm with a treponemal test and review the VDRL or RPR titer with your clinician.
I am allergic to penicillin. What now?
There are alternatives for nonpregnant patients. In pregnancy, penicillin is the standard. Desensitization is recommended so penicillin can be given safely.
After treatment, can I get infected again?
Yes. Treatment does not confer immunity. Prevention and periodic testing remain important.
Important notice (health disclaimer)
This content is educational and does not replace medical care. For individualized diagnosis, treatment, and follow-up, seek professional evaluation. In pregnancy, prompt management is critical to prevent congenital syphilis.
References and recommended reading
CDC. Sexually Transmitted Infections Treatment Guidelines: Syphilis.
WHO. Guidance on syphilis screening and treatment in pregnancy and the general population.
PAHO. Elimination of mother-to-child transmission of syphilis: recommendations.
Cochrane Reviews. Antibiotic regimens for early and late syphilis.
ECDC. Syphilis surveillance and public health guidance.
National infectious diseases and obstetrics–gynecology societies. Guidelines for screening and management in pregnancy.