Content discussed in this post
What cancer is and key terms
Benign vs malignant: what changes in practice
Metastasis: how cancer spreads
Staging: TNM and clinical stages
How to read survival statistics with sensitivity
Treatments: surgery, chemotherapy, radiotherapy, targeted therapies, immunotherapy, and integrated palliative care
Common cancers in focus: testicular, breast, prostate, lung cancer, and melanoma
Quick myths and clarifications
Quick FAQ
Important notice (health disclaimer)
References and recommended reading
What cancer is and key terms
Cancer happens when the body’s cells lose growth control and start multiplying in a disorganized way. By invading nearby tissues and escaping through blood or lymphatic vessels, these cells can settle in other organs. It is a disease of the body itself, not something “from outside,” which is why it often requires a strategy that combines surgery, medicines, and supportive care.
Benign vs malignant: what changes in practice
A benign tumor grows locally, usually has clear boundaries, and, in general, does not invade nearby structures or metastasize. It can cause symptoms due to size or location, but its behavior is less aggressive.
A malignant tumor (cancer) invades tissue, can infiltrate nerves and vessels, and has the potential to metastasize. Diagnosis depends on a biopsy and laboratory analysis, which also identify tumor characteristics that help plan treatment.
Important: a lump you can feel is not always cancer. Cysts, lipomas, and inflammatory processes are common. The real difference comes from medical evaluation.
Metastasis: how cancer spreads
Metastasis means cells from the original tumor have reached another organ and begun to grow there. The most frequent routes are:
Lymphatic, passing through lymph nodes
Hematogenous, via the bloodstream to lungs, liver, bones, or brain
By contiguity, when the tumor extends directly into neighboring structures
Important example: breast cancer with bone metastasis is still breast cancer. The origin defines the biology and guides therapy.
Staging: TNM and clinical stages
For solid tumors, the most used system summarizes three pieces of information:
T for the primary tumor, its size, and local extent
N for involved regional lymph nodes
M for distant metastasis
Combining T, N, and M yields the clinical stage. In broad terms:
Stage 0 is very early disease, in situ
Stage I is small and localized
Stage II is usually larger and may involve a few lymph nodes
Stage III indicates more extensive regional involvement
Stage IV means distant metastasis
Some cancers follow their own schemes. Testicular cancer, for example, classifies disseminated disease as stage III, with international prognostic groups that guide chemotherapy. In everyday conversation, you may hear “stage 4” for any metastatic cancer. Although the official term in testicular cancer is stage III, what truly determines the plan is the prognostic group and response to chemotherapy regimens.
How to read survival statistics with sensitivity
Numbers help frame the landscape, but they do not define a person’s fate. Keep a steady mind and a calm heart with a few reminders:
Statistics describe groups, not individuals. There is wide variation among people with the same diagnosis.
Results change over time. Modern therapies have improved survival in several tumors, including advanced disease.
Tumor biology and response to treatment matter greatly. Two tumors in the same organ can behave differently.
Integrated care with nutrition, tailored physical activity, symptom control, and mental health support influences quality of life and adherence to treatment.
When you receive a number, use it as a broad reference. The practical focus is to keep appointments, address controllable factors, manage side effects, and follow the plan agreed upon with the care team.
Treatments: overview
Treatment is designed by a multidisciplinary team.
Surgery removes the tumor when possible. It can be curative in early stages or part of a broader plan.
Radiotherapy controls local disease and, in some scenarios, helps prevent recurrences.
Chemotherapy uses systemic medicines that target dividing cells. It is given in cycles with breaks for recovery. Nausea, hair loss, and fatigue are common effects, now better controlled with supportive medications. In younger people, it is important to discuss fertility preservation before starting.
Targeted therapies act on specific tumor alterations. They depend on tests performed on biopsy material.
Immunotherapy helps the immune system recognize cancer cells. It has brought gains in tumors such as lung cancer and melanoma.
Integrated palliative care starts early in modern oncology. It does not mean “giving up.” It means relieving symptoms, supporting decisions, and protecting quality of life in any phase.
Common cancers in focus
Testicular cancer
Most are germ cell tumors and respond very well to platinum-based chemotherapy. Even with disseminated disease, cure rates are high in many cases. Treatment follows well-established protocols, and prognosis considers a risk group defined by blood tests and sites of metastasis. The central message is aggressive treatment with curative intent when clinically appropriate.
Breast cancer
It is not a single disease. Biological subtype matters: hormone receptors, HER2, and additional markers define options. In early stages, surgery plus radiotherapy and, when indicated, endocrine therapy, chemotherapy, and anti-HER2 therapies yield excellent outcomes. In advanced disease, multiple treatment lines aim to control cancer and preserve quality of life for long periods.
Prostate cancer
Many tumors grow slowly. Management ranges from active surveillance to surgery and radiotherapy. In advanced disease, hormonal blockade and newer options such as radioligand therapies and PARP inhibitors in selected profiles have expanded choices. Managing urinary symptoms, bone health, and tailored physical activity are part of care.
Lung cancer
Progress has been significant with molecular testing and immunotherapy. Identifying mutations and rearrangements in the tumor opens doors to targeted therapies that improve survival and symptoms. Smoking cessation, when relevant, improves response and reduces complications. Pulmonary rehabilitation and nutritional support help day to day.
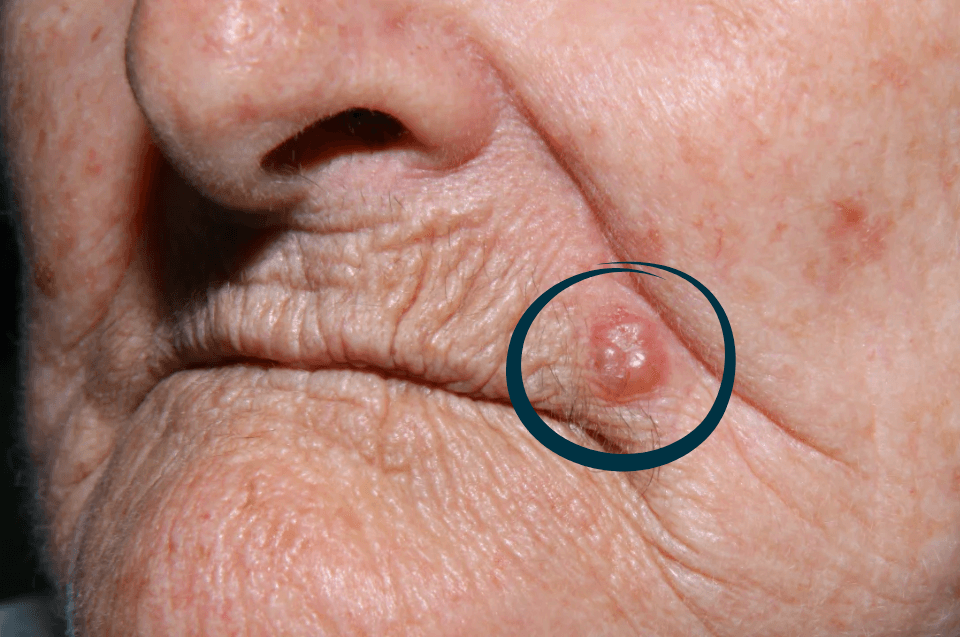
Melanoma
The major shift came with immunotherapy and, in subgroups, targeted therapies. In early stages, surgery is the focus. In advanced disease, durable responses have become a reality for a portion of patients. Sun protection and skin surveillance remain important for everyone.
Quick myths and clarifications
“Metastasis is always the end.” Not true for several tumors. In some, there is curative intent even with disseminated disease.
“Biopsy spreads cancer.” Procedures performed with proper technique are safe and do not increase metastasis.
“Every lump is cancer.” Many nodules are benign. Proper investigation is the way to avoid false alarms.
Quick FAQ
Does stage 4 always mean metastasis?
For most solid tumors, yes. Some types use different nomenclature, such as testicular cancer, but metastasis means systemic disease that requires specific treatment.
How long does chemotherapy last?
It depends on the protocol and the goal. Some regimens last a few months; others are given continuously. The team adjusts according to response and tolerance.
Is it possible to live well with advanced cancer?
Yes. With modern therapies and integrated support, many people maintain routines, relationships, and projects even while in treatment.
Important notice (health disclaimer)
This content is educational and does not replace medical consultation. Diagnosis, staging, and treatment must be defined by a specialized team based on biopsy, imaging, and the characteristics of the tumor and the individual.
References and recommended reading
INCA. Basic concepts, staging, and management guides.
SEER/NIH. Statistics by type and stage, survival methodology.
WHO/IARC (GLOBOCAN). Global incidence and mortality.
NCCN. Site-specific guidelines.
ESMO. European clinical practice guidelines.
American Cancer Society. Materials for patients and caregivers.
National societies of medical oncology, radiation oncology, pathology, and surgical oncology.